Umbilical (belly button) and para-umbilical hernia repair
A hernia is an abnormal protrusion on an organ through a weakness in the abdominal wall. There is a natural weakness in the abdominal wall at the umbilicus, caused by the way babies develop in the womb. If the contents of the abdomen push through, this produces a lump called a hernia. It can either be directly through the center or the umbilicus, termed an umbilical hernia, or beside the umbilicus, termed a para-umbilical hernia. Straining, for example on the toilet or lifting heavy weights, increases pressure inside the abdomen and can trigger a hernia.
Why is it necessary to operate on an inguinal hernia?
Most people with a hernia present with pain and repairing the hernia will alleviate the pain. In addition a hernia is potentially dangerous as the herniated bowel may become incarcerated leading to bowel obstruction or strangulation as a result of the blood supply to the bowel being compromised. Only surgery can repair the hernia, they will not go away on their own.
How is the hernia repaired?
Surgery to repair paraumbilical and umbilical hernias is usually performed under a general anaesthetic but can be done under local with sedation if necessary. The operation usually takes about 30 minutes. A small incision is made either above or below your umbilicus. The hernia is pushed back into the abdomen and the defect in the abdominal wall that allowed for the abdominal contents to protrude out is closed either with strong non-absorbable stitches or placement of a synthetic mesh.
What are the main risks with having the hernia repaired?
Abdominal hernia repair is a routine operation with very few risks, however all surgery has some risks. Complications occur in about 5% of cases and most are mild and easily resolved. The principal risks include recurrence, wound infection or hematoma (blood collection) and seroma (clear tissue fluid collecting in the space left by the hernia). In some instances if the hernia is large, the umbilicus may need to be resected, leaving you with a incision and no belly button. General risks of surgery includes, wound infection, unsightly scaring, deep vein thrombosis (DVT) or pulmonary embolism. There is an increased risk of post- operative complications if you are overweight or if you smoke.
What tests are done?
Most patients do not require any radiological tests. The diagnosis is made by clinical examination.
You may require routine blood tests prior to the operation as part of your anaesthetic workup
Are there any alternatives?
There are no other effective treatments for the management of inguinal hernia. If the hernia is small and does not cause you any discomfort, then leaving it alone may be entirely appropriate. Some people wear supports (trusses or corsets) to hold their hernia in. These devices are not recommended as they may cause more harm than good. There may be certain situations where your doctor may think wearing a support is a better option, but this is rare. This usually relates to the presence of other medical issues. In that instance alternative treatment strategies may be discussed.
How long will I be in hospital?
Most patients will come into hospital on the day of their operation, and will be able to go home later the same day (day stay). If there is any issue with pain control or ability to pass urine, you may be kept in over night.
What happens before the operation?
Prior to the operation you will be asked to complete an anaesthetic questioner. This will be passed onto the anesthetist that will be looking after you during the operation. Depending upon your medical status you may require an assessment or other investigations. You will need to have bloods taken in the recent weeks prior to surgery, and these may need to be repeated. You will be given specific instructions about when to stop eating and drinking, please follow these carefully as otherwise this may pose an anaesthetic risk and we may have to cancel your surgery. You should bath or shower before coming to hospital as you normally would. You do not need to shave any of the abdominal or pubic hair. You should take all your normal medication even on the day of surgery with a small amount of water. If you are on any medication that affects blood clotting you need to let the surgeon know well in advance of your surgery, as they may need to be stopped.
What happens when I arrive at the hospital?
You will be seen by the nursing staff and taken to your room. You will be asked to change into a theatre gown. The surgeon and anaesthetist will visit you and answer any questions that you have.
You will be asked to sign a consent form, and the surgeon will mark the operative site with indelible ink to avoid any potential confusion. You will be taken into the operating room by a nurse who will with you until you are asleep.
What happens after the operation?
You will be woken in the operating room after the operation has been completed, and taken into the recovery area. You will have an intravenous line in you arm that is attached to fluid, and enables the staff to give you medication. You will have an oxygen mask over your mouth that will administer supplemental oxygen. A blood pressure cuff will be on one of your arms, and intermittently inflate to measure you blood pressure. You will be able to eat and drink as soon as you are hungry after the procedure. You will normally be able to get out of bed a few hours after surgery although the nurses will assist you the first time.
How much pain will I experience post-operatively?
Most people only experience mild-to-moderate pain, which is readily controlled with oral analgesia (painkillers). You may experience some pain from your incisions, especially on movement. If you do, the nurses will give you analgesia. At the time of discharge you will be given a supply of painkillers and post-operative instructions on what to take when. After about 7 days most of the discomfort should disappear.
How long will it take to recover from the anaesthetic?
Whilst most of the effects of anaesthesia wear off in a few hours, it is common to have poor concentration and memory for a few days thereafter. It is important that you do not make important
decisions, sign legal documents or operate machinery or equipment for at least 24 hours after the general anaesthetic. You will not be able to drive home from the hospital, so you will need to make arrangements for someone to pick you up, and be available to keep an eye on you over night.
When can I return to normal activities?
You can return to normal physical and sexual activities when you feel comfortable. It is normal to feel tired after surgery, so take some rest, two or three times a day, and try to get a good nights sleep. After a week or so, you should be able to resume your normal daily activities. You should avoid any heavy lifting (more than 6kg) or straining for 6 weeks after the operation.
When can I start driving?
You should not drive for at least 48 hours after the laparoscopy. Before driving you should ensure that you could perform a full emergency stop, have the strength and capability to control the car, and be able to respond quickly to any situation that may occur. Please be aware that driving whilst unfit may invalidate your insurance, and you should check with the conditions of your insurance policy as they do vary
When can I return to work?
You can return to work as soon as you feel up to it. This will depend on how you are feeling and the type of work that you do. If you have a relatively sedentary job then you may feel ready to return within 3-4 days. If you are involved in manual labor or heavy lifting you need to remain on light duties for at least 6 weeks.
What can I eat?
There are no dietary restrictions after repair of your inguinal hernia and you may resume a normal diet as soon as you are hungry. It may take a few days before your appetite returns. When you feel hungry start with light frequent meals and then increase at your own pace.
When will my bowel movements return to normal?
It may take three or four days to have a normal bowel movement. If you have not had a bowel movement three days after surgery, a mild laxative should help. Alternatively Alpine tea, prune juice or kiwifruit may be equally effective. I
How do I care for my wounds?
The dressings are usually changed the following morning, and we leave them undisturbed until you are seen the following week. It is not an issue taking a shower, they can get wet, but avoid soaking in the bath. If they do fall off then there is no need to replace them unless you feel it is more comfortable. Steri-strips are placed over the incision sites under the dressings. These will usually fall off within a week or so. If any are still in place after a week you can gently remove them. The incisions are closed with dissolvable stitches that do not need to be removed. The incisions will probably be red and uncomfortable for 1-2 weeks and some bruising and swelling is common. After the incisions have healed there will be a small, scar like scratch. It is ok to use Bio-oil on the incisions after the first week to help reduce scar prominence.
When should I seek help?
If you have concerns then either ring the surgeon directly or the hospital for advice. If it is medical emergency then dial 111 for an ambulance to take you to an acute hospital. You should let us know if you have a discharge of blood or pus coming from your wounds, develop a fever over 38.5 ° C, vomiting that continues more than three days after surgery, inability to have a bowel movement after four days, have persistent pain not relieved with your prescribed painkillers or persistent abdominal distension (bloating of your tummy), develop increasing pain or swelling around your wounds.
 A hernia occurs when the inside layers of the abdominal muscle have weakened, resulting in a bulge or tear. In the same way that an inner tube pushes through a damaged tyre, the inner lining of the abdomen pushes through the weakened area of the abdominal wall to form a small balloon-like sac. This can allow a loop of intestine or abdominal tissue to push into the sac. The hernia can cause severe pain and other potentially serious problems that could require emergency surgery. You may be born with a hernia (congenital) or develop one over time. A hernia does not get better over time, nor will it go away by itself.
A hernia occurs when the inside layers of the abdominal muscle have weakened, resulting in a bulge or tear. In the same way that an inner tube pushes through a damaged tyre, the inner lining of the abdomen pushes through the weakened area of the abdominal wall to form a small balloon-like sac. This can allow a loop of intestine or abdominal tissue to push into the sac. The hernia can cause severe pain and other potentially serious problems that could require emergency surgery. You may be born with a hernia (congenital) or develop one over time. A hernia does not get better over time, nor will it go away by itself. The common areas where hernias occur are in the groin (inguinal), belly button (umbilical), and the site of a previous operation (incisional). It is usually easy to recognize a hernia. You may notice a bulge under the skin. You may feel pain when you lift heavy objects, cough, or strain during urination or bowel movements, or during prolonged standing or sitting. The bulge usually comes and goes depending on activities. The pain may be sharp and immediate or a dull ache that gets worse toward the end of the day.
The common areas where hernias occur are in the groin (inguinal), belly button (umbilical), and the site of a previous operation (incisional). It is usually easy to recognize a hernia. You may notice a bulge under the skin. You may feel pain when you lift heavy objects, cough, or strain during urination or bowel movements, or during prolonged standing or sitting. The bulge usually comes and goes depending on activities. The pain may be sharp and immediate or a dull ache that gets worse toward the end of the day.

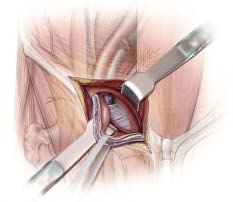 The most commonly performed inguinal hernia repair today is the Lichtenstein or open anterior mesh repair. A flat mesh is placed on top of the defect. It is a “tension-free” repair that does not put tension on muscles. It involves the placement of a mesh to strengthen the inguinal region. Patients typically go home within a few hours of surgery, or the following day and often require little pain medication. ©Compiled by the Hernia Interest Group, SASES, 2015
The most commonly performed inguinal hernia repair today is the Lichtenstein or open anterior mesh repair. A flat mesh is placed on top of the defect. It is a “tension-free” repair that does not put tension on muscles. It involves the placement of a mesh to strengthen the inguinal region. Patients typically go home within a few hours of surgery, or the following day and often require little pain medication. ©Compiled by the Hernia Interest Group, SASES, 2015

 Following the operation, you will be transferred to the recovery room where you will be monitored for 1-2 hours until you are fully awake. Once you are awake and able to walk and are able to freely pass urine, you may be sent home, although some hospitals keep patients overnight. With any hernia operation, you can expect some soreness mostly during the first 24 to 48 hours. You are encouraged to be up and about the day after surgery.With laparoscopic hernia repair, you will probably be able to get back to your normal activities within a short amount of time. These activities include showering, driving, walking up stairs, lifting, working and engaging in sexual intercourse. Recovery after open surgery takes a little longer, but you should be able to do most things as normal within 2 weeks. ©
Following the operation, you will be transferred to the recovery room where you will be monitored for 1-2 hours until you are fully awake. Once you are awake and able to walk and are able to freely pass urine, you may be sent home, although some hospitals keep patients overnight. With any hernia operation, you can expect some soreness mostly during the first 24 to 48 hours. You are encouraged to be up and about the day after surgery.With laparoscopic hernia repair, you will probably be able to get back to your normal activities within a short amount of time. These activities include showering, driving, walking up stairs, lifting, working and engaging in sexual intercourse. Recovery after open surgery takes a little longer, but you should be able to do most things as normal within 2 weeks. ©